Campus updates
Can SA’s achievement in containing COVID-19 lead to sustained success?
28 April 2020 | Story Alan Hirsch. Photo: Wikimedia Commons. Read time 6 min.
South Africa has been recognised globally for its success in flattening the curve, which came as a result of President Ramaphosa listening to experts and responding quickly with social distancing introduced on 15 March and a nationwide lockdown on 27 March, writes the University of Cape Town’s Professor Alan Hirsch.
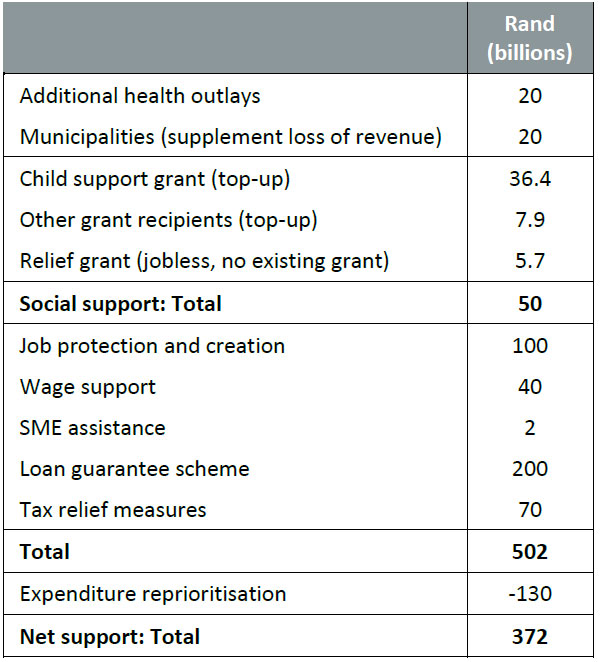
On April 21st, President Ramaphosa announced a huge economic support programme designed to assist the vulnerable poor and sustain small and medium businesses in distress. The package is valued at R500bn or $25bn, including R200bn in credit guarantees and R130bn through reprioritisation of the budget. Some of the funds will also come from the Unemployment Insurance Fund. It is a massive package by South African standards at 10 percent of GDP or a third of the annual budget. The package has been widely acclaimed, almost across the entire political spectrum. It is pro-poor and pro-formal sector employee; and supports businesses through SME support, a job creation and retention fund, as well as through credit support.
President Ramaphosa has also been acclaimed for his continental leadership as Africa’s G20 member and as Chair of the African Union. Working with the Chair of the AU commission, he has established a strong team of African financial leaders to lobby for the continent across the financial community.
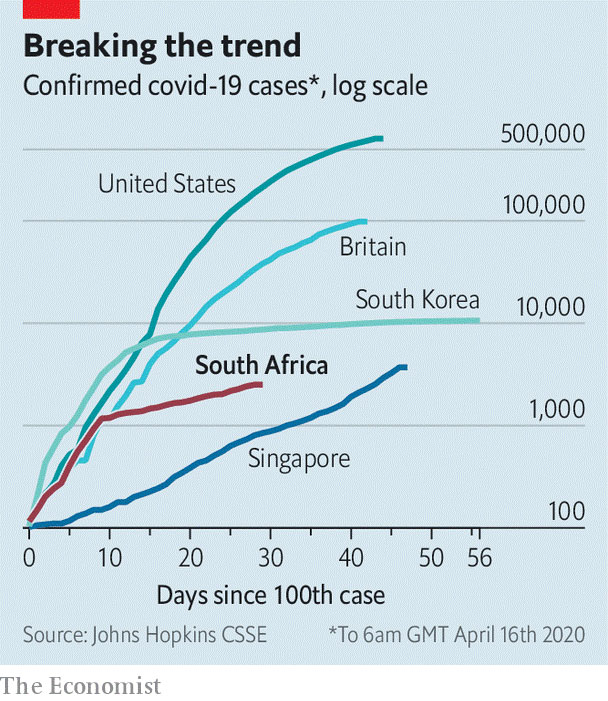
South Africa has been recognised globally for its success in flattening the curve. On April 16th, The Economist reported that in South Africa “in the week to March 28th the number of confirmed cases quadrupled. But it took 17 days for the reported tally to double after that date. What looked at first like a Britain-style trajectory has come to appear more like South Korea’s (see chart).” This was a result of President Ramaphosa listening to experts and responding quickly with social distancing introduced on March 15th and a lock-down on March 27th.
Success in flattening the curve has been the result of a strict “level 5” lockdown, prior to the easing of restrictions on April 23rd “to level 4”. South Africans have been allowed to go outside of their homes to buy essentials or for medical needs, but not to exercise or walk the dog. The sale of alcohol is banned, as well as cigarettes and “cooked hot food” (the latter two to be lifted on Friday). The streets are largely deserted except for a few of the homeless poor who have evaded efforts to corral them into emergency camps for safety purposes. A number of these measures have been faced with legal challenges: one court case contested the ban on the sale of cigarettes; another the ban on the sale of cooked hot food. Both court actions have derived from the extreme restrictiveness of the South African lockdown.
The rationale for this tough regime in South Africa (and in some other developing countries) is a lack of confidence in the national capacity to treat and cure COVID-19 and other patients. Compared with developed countries, most developing countries also have poorer testing capacities and weaker tracing systems. However, compared with many other developing countries South Africa has the (dubious) advantage of having driven a huge public health initiative to combat the spread and impact of HIV/AIDS. It has skills, knowledge and systems, but the capacity of the health system and access to intensive care and assisted breathing facilities are still limited.
The strictness of the lockdown has evolved into a paternalistic approach that has verged on control-freakishness. There have been several cases of excessive force used by police and soldiers who conduct patrols to enforce the lock-down. Level 4 includes a 9-hour curfew from 20.00 to 05.00, with a recently increased call out of the defence force, presumably to enforce the curfew.
This could be a result of a trust deficit between government and citizens. Francis Fukuyama has argued that the difference between successful “flatten the curve” initiatives and weaker outcomes is not explained by the authoritarian/liberal divide, but by the degree of confidence of citizens in the competence of their government and the quality of leadership. While President Ramaphosa’s already high popularity rating seems to have risen as a result of his decisive responses to the crisis, the trust of South African citizens in government and political parties is considerably lower. It may be knowledge of the lack of trust in government institutions that has led to the paternalistic behaviour by many parts of government.
The extreme lockdown also raised huge questions of welfare and economic sustainability. 42 percent of firms responding to a new national survey indicated that they doubted they could survive the lockdown. Sixty-six percent of respondents to another new national survey were struggling to pay their expenses and 28 percent indicated that they had gone to bed hungry since the lockdown began. Many children relied on a wide-scale school-feeding scheme, which was stopped when the schools closed, and many poor providers relied on precarious sources of income, that they have been unable to tap. While 70 percent of the middle classes were comfortable with a continuation of the lock-down, only 35 percent of the very poor agreed.
The capacity of the government to intervene is limited financially when the government is under severe financial stress, with a wide range of heavily indebted institutions including the Land Bank (the state agricultural bank) which defaulted on a loan on April 21. This follows a series of downgrades of South African government debt well into junk grade before the COVID-19 crisis struck. This was a result of mismanagement of government and government agency finances for many years which the Ramaphosa government has as yet been unable to reverse. Many developing countries are indebted and few are able to raise additional funds at anything but extortionate rates, except for the limited amount of concessional finance currently available. Some financial analysts are concerned that South Africa may already be relying too much on cash it doesn’t have to address the crisis.
Even if South Africa and other developing countries had more funds, channelling those funds to the neediest is very difficult. South Africa has a strong system of social transfers, but many in the informal sector will not be reached through it. For all these reasons, the issue of phasedown is very urgent in South Africa, as it is in other developing countries. Some moved quicker – Ghana lifted its lockdown of two cities after three weeks, citing its severe impact on the poor and improved testing capabilities. Though the Indian lockdown was extended to May 4th, from April 20th low risk zones known as green zones had some restrictions removed.
The new budget and the debt it will incur, make it all the more urgent that the economy begins operating at a higher level soon, and that economic growth is raised above pre-crisis levels. The next step is the judicious “risk-adjusted “phasing down of the lockdown. With its repurposed HIV/AIDS testing systems, South Africa is currently testing more than 9,000 people per day, with a total of 178,470 tested by April 27th. This should make the process of conducting carefully managed, constantly evaluated phasing in of increased economic activity possible in the near future. It will also need a further adjustment of attitudes between state and citizens away from paternalism and compliance towards trust and cooperation.
Alan Hirsch, Professor of Development Policy and Practice at The Nelson Mandela School of Public Governance at University of Cape Town.





UCT’s response to COVID-19
COVID-19 is a global pandemic that caused President Cyril Ramaphosa to declare a national disaster in South Africa on 15 March 2020 and to implement a national lockdown from 26 March 2020. UCT is taking the threat of infection in our university community extremely seriously, and this page will be updated with the latest COVID-19 information. Please note that the information on this page is subject to change depending on current lockdown regulations.
Minister of Health, Dr Joe Phaahla, has in June 2022 repealed some of South Africa’s remaining COVID-19 regulations: namely, sections 16A, 16B and 16C of the Regulations Relating to the Surveillance and the Control of Notifiable Medical Conditions under the National Health Act. We are now no longer required to wear masks or limit gatherings. Venue restrictions and checks for travellers coming into South Africa have now also been removed.
Read the latest document available on the UCT policies web page.
Campus communications
2022
UCT Community of Hope Vaccination Centre
On Wednesday, 20 July, staff from the University of Cape Town’s (UCT) Faculty of Health Sciences came together with representatives from the Western Cape Government at the UCT Community of Hope Vaccination Centre at Forest Hill Residence to acknowledge the centre’s significance in the fight against COVID-19 and to thank its staff for their contributions. The centre opened on 1 September 2021 with the aim of providing quality vaccination services to UCT staff, students and the nearby communities, as well as to create an opportunity for medical students from the Faculty of Health Sciences to gain practical public health skills. The vaccination centre ceased operations on Friday, 29 July 2022.
With the closure of the UCT Community of Hope Vaccination Centre, if you still require access to a COVID-19 vaccination site please visit the CovidComms SA website to find an alternative.


“After almost a year of operation, the University of Cape Town’s (UCT) Community of Hope Vaccination Centre, located at the Forest Hill residence complex in Mowbray, will close on Friday, 29 July 2022. I am extremely grateful and proud of all staff, students and everyone involved in this important project.”
– Vice-Chancellor Prof Mamokgethi PhakengWith the closure of the UCT Community of Hope Vaccination Centre, if you still require access to a COVID-19 vaccination site please visit the CovidComms SA website to find an alternative.
Frequently asked questions


Global Citizen Asks: Are COVID-19 Vaccines Safe & Effective?
UCT’s Institute of Infectious Disease and Molecular Medicine (IDM) collaborated with Global Citizen, speaking to trusted experts to dispel vaccine misinformation.






If you have further questions about the COVID-19 vaccine check out the FAQ produced by the Desmond Tutu Health Foundation (DTHF). The DTHF has developed a dedicated chat function where you can ask your vaccine-related questions on the bottom right hand corner of the website.
IDM YouTube channel | IDM website
“As a contact university, we look forward to readjusting our undergraduate and postgraduate programmes in 2023 as the COVID-19 regulations have been repealed.”
– Prof Harsha Kathard, Acting Deputy Vice-Chancellor: Teaching and Learning
We are continuing to monitor the situation and we will be updating the UCT community regularly – as and when there are further updates. If you are concerned or need more information, students can contact the Student Wellness Service on 021 650 5620 or 021 650 1271 (after hours), while staff can contact 021 650 5685.