Wamkelekile, Welkom
Making a case for investing in mental health
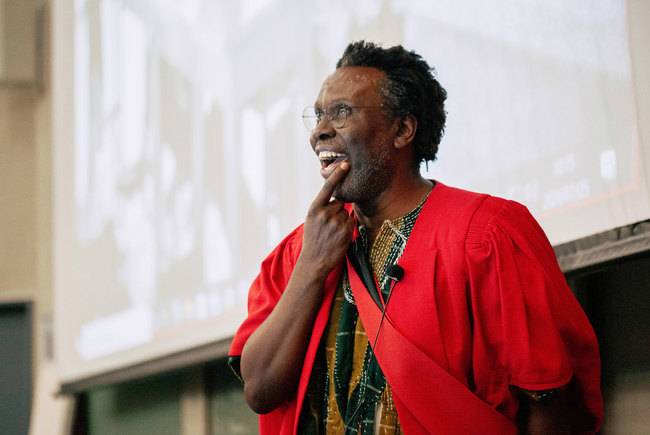
25 May 2018 | Story Penny Haw. Photo Je’nine May Read time 8 min.
Drawing on his research and policy engagement work over the past two decades, Professor Crick Lund presented a compelling case for investing in population mental health during his inaugural lecture in the New Learning Centre on 23 May.
Lund is Professor of Public Mental Health in UCT's Department of Psychiatry and Mental Health. He is a leading researcher in mental health care and developing mental health policies and services that address the growing burden of mental illness in South Africa and other low- and middle-income countries.
His lecture, titled “Ten reasons to invest in population mental health in low- and middle-income countries”, underscored his interest in creating public awareness by highlighting the links between poverty and mental illness, and by exploring ways to break this cycle with his research.
After describing how his career evolved – Lund is, among many other things, a founding member of the Alan J Flisher Centre for Public Mental Health, which is a UCT Research Centre and World Health Organization (WHO) Collaborating Centre in the Department of Psychiatry and Mental Health – he provided several key definitions to give context to the reasons for investing in mental health.
Complex social and cultural determinants
In illustrating the complexity of social and cultural determinants in relation to mental health, Lund showed a map of the Western Cape and described the factors that drive population mental health in the province.
The region, he pointed out, includes the winelands, which have been affected by both the dop system and foetal alcohol syndrome, and the Cape Flats where the use of tik (crystal methamphetamine) is prevalent. Other factors that influence mental health in the Western Cape, particularly in poor communities, are inadequate water and sanitation, inferior housing, inequality, violence, food insecurity, unemployment and migratory challenges.
The key questions, said Lund, are where do you go for help if you are psychotic or suicidal and live in disadvantaged communities, where do you find services and why are services organised in the way they are?
The significance of considering these issues is that it encourages clinicians to shift their thinking beyond individual cases to systems, services and communities – crucial to understanding and evaluating population mental health.

The reasons
Lund’s 10 reasons to invest in population mental health in low- and middle-income countries are summarised as follows:
- burden of disease
- no health without mental health
- lack of policy commitment and resources – the treatment gap
- social and economic costs of mental illnesses
- cycle of poverty and mental illness
- human rights
- links between mental health and the United Nations Sustainable Development Goals (SDGs)
- policy, planning and legislation guidelines and tools are available
- cost-effective interventions and low-cost service models are available
- return on investment – it pays to invest in mental health care.
At the top of Lund’s reasons to invest in population mental health in low- and middle-income countries is the burden of mental disorders. The Global Burden of Disease Study (1990–2015), he said, documents the burden of mental disorders in relation to other health conditions and shows a consistent trend in regions around the world of a growing burden of mental and substance abuse disorders.
“When we looked at [the study] we also saw that the distribution of these disorders is not even across the life course,” said Lund. “There’s a spike in adolescence and early adulthood, which places young people at particular risk, especially for conditions like depression, anxiety and substance abuse.
“This is a critical developmental stage, which often sets a trajectory for lifelong development and economic productivity.”
The second reason Lund gave is that there is “no health without mental health”. He discussed issues of comorbidity, including research which shows that people with mental disorders are at increased risk of contracting HIV or AIDS and that among HIV-positive individuals, the prevalence of mental disorders is higher than it is in the general population.
Studies have also found that treating depression improves antiretroviral therapy adherence and CD4 (cluster of differentiation 4) count.
“Despite the massive burden and despite the high levels of comorbidity with other health conditions and the opportunity to provide treatment for mental health that will also improve other health outcomes, there is a major lack of policy commitment and resources.”
This leads to investment motive three, “what we know as the treatment gap”.
“Despite the massive burden and despite the high levels of comorbidity with other health conditions ... there is a major lack of policy commitment and resources.”
The fourth reason is the social and economic costs of mental illness. Here, Lund cited several studies, including one that showed “anxiety disorders and depression were associated with the highest ‘days out of role’ (that is, a measure of inability to work or carry out day-to-day activities) out of all mental and physical illnesses, at 28.2 and 27.2 days per year respectively”.
The cycle of poverty and mental illness was listed as the fifth reason, with Lund explaining that one of the big challenges is understanding causality.
“At a very basic level, we ask whether people are depressed because they are poor or poor because they are depressed,” he said, explaining that several studies indicate that both are true, which is why the cycle prevails.
Lund’s sixth reason for investing in population mental health is that it is a human right. He briefly discussed the tragic Life Esidimeni case, which resulted in the deaths of 143 mentally ill patients because of mismanagement and poor use of resources during 2015 and 2016.
Links between mental health and the United Nations SDGs came in as reason number seven with obvious correlation to SDG three (‘Good health and well-being’). But, in fact, as Lund pointed out, presenting a recently published framework for linking them, the social determinants of mental health correspond with all of the other 16 SDGs.
The availability of policy, planning and legislation guidelines and tools is a further reason (number eight) to invest in population mental health, he said, describing several examples of work done in this regard by his colleagues.
Closely associated to this is the ninth reason: “We have cost-effective interventions and low-cost service models.”

Among these are the PRIME (Programme for Improving Mental Health Care) initiative, which is a Department for International Development-funded consortium of research institutions and ministries of health in Ethiopia, India, Nepal, South Africa and Uganda, with partners in the United Kingdom and the WHO, and AFFIRM (Africa Focus on Intervention Research for Mental Health).
Lund’s 10th and final motive might be considered the most persuasive: “Return on investment – it pays to invest in mental health care.”
He cited the findings of the 2016 study led by Dan Chisholm of the WHO, which found that for every dollar spent on improving treatment for depression and anxiety, the return on the investment could be fourfold or higher in terms of increased productivity and health.
“Very encouragingly, the World Bank and the WHO expressed their commitment to mental health at a meeting called Out of the Shadows, which aimed to bring mental health from the periphery to the centre of the global development agenda,” said Lund.
 This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Please view the republishing articles page for more information.





The UCT Inaugural Lecture Series
Inaugural lectures are a central part of university academic life. These events are held to commemorate the inaugural lecturer’s appointment to full professorship. They provide a platform for the academic to present the body of research that they have been focusing on during their career, while also giving UCT the opportunity to showcase its academics and share its research with members of the wider university community and the general public in an accessible way.
In April 2023, Interim Vice-Chancellor Emeritus Professor Daya Reddy announced that the Vice-Chancellor’s Inaugural Lecture Series would be held in abeyance in the coming months, to accommodate a resumption of inaugural lectures under a reconfigured UCT Inaugural Lecture Series – where the UCT extended executive has resolved that for the foreseeable future, all inaugural lectures will be resumed at faculty level.
Recent executive communications
2026

Professor Elena Moore of the Department of Sociology at the University of Cape Town delivered her inaugural lecture on 4 March, titled: “Who Cares? The Directions of State–Family Relationships in Changing Times”. The lecture drew together more than two decades of research into how families and societies organise, experience, and govern care.
09 Mar 20262025


At the heart of modern finance is a question of trust. What happens when the systems built to uphold it begin to falter? The lecture by Professor Phillip de Jager in the Department of Finance and Tax at the University of Cape Town (UCT) explored this thought.
11 Nov 2025













2024




















Professor Susan Cleary delivered her inaugural lecture on 14 March.
14 Mar 2024 - 5 min read
2023


Prof Lydia Cairncross’s inaugural lecture provided a snapshot of the career path of a surgeon and community activist whose commitment to social justice means her work doesn’t end in the operating theatre.
02 Nov 2023 - 8 min read









2022

Professor Linda Ronnie is in UCT’s Faculty of Commerce.
28 Sep 2022 - 6 min read
.jpg)

2021

2020
2019





2018







2017


2016 and 2015
No inaugural lectures took place during 2015 and 2016.