Wamkelekile, Welkom
How the stressful crush of emergency remote teaching became an all-time career highlight
09 December 2020 | Story Chivaugn Gordon. Photo Je’nine May. Read time 4 min.
Dr Chivaugn Gordon, Head of Undergraduate Obstetrics & Gynaecology Education embraced the drastic shift to Emergency Remote Teaching with great chutzpah.
“Emergency Remote Teaching”. What was that, even? We were all left reeling under lockdown, fearing for our and our loved ones’ safety and sanity, but also needing to create content from scratch for our students. We were overwhelmed with unknowns, but there were a few things I did know. As a medical educationist with an MPhil in Health Professions Education, I have a detailed knowledge of what makes a good teaching & learning experience, but so far, this had only applied in face-to-face settings. I felt very strongly that I still wanted my students to have a really good, high quality, enjoyable and fun experience, despite not being in the room with their teachers. I will mainly reflect on the content that I made myself in this piece, but some background information is needed.
I had never designed an online course before, yet our Department was now expected to create four Emergency Remote Teaching courses, two of which I was directly responsible for. I was reasonably familiar with Vula (the University’s online learning and collaboration system), but I had never fully built a website. So what did I do?
 Firstly, I didn’t and couldn’t do it alone. The Centre for Innovation and Learning in Teaching (CILT) provided excellent guidelines as to how a website should be structured. This included creating a clear pathway for students to progress, so the content was broken up into weeks and days, which students really appreciated. Furthermore, I considered the massive student survey which stated that the average time that most students could spend online per day was about 4-5 hours. I had to be brutally realistic about what was achievable on a given day (knowing that I could be wrong!). CILT also advised on maximum file sizes, and that all video content needed to be transcribed. These were adhered to, and again, much appreciated by the students. Having some basic logistics clear, we needed to decide who would make the content.
Firstly, I didn’t and couldn’t do it alone. The Centre for Innovation and Learning in Teaching (CILT) provided excellent guidelines as to how a website should be structured. This included creating a clear pathway for students to progress, so the content was broken up into weeks and days, which students really appreciated. Furthermore, I considered the massive student survey which stated that the average time that most students could spend online per day was about 4-5 hours. I had to be brutally realistic about what was achievable on a given day (knowing that I could be wrong!). CILT also advised on maximum file sizes, and that all video content needed to be transcribed. These were adhered to, and again, much appreciated by the students. Having some basic logistics clear, we needed to decide who would make the content.
My team of undergraduate teachers really stepped up to the challenge, but I also involved some volunteer students in content creation, site construction and other logistics. I was truly amazed at what this collaboration allowed, and the student voice was invaluable.
While we did make use of some narrated Power Points, most of the content that I made was in video format. I had no idea how to achieve making my own videos - would my phone be adequate, how would I transfer the videos, how would I hold it up? A fellow educationist colleague told me that all I needed was a tripod and my phone, and my colleague and I managed to grab two dirt-cheap tripods just before lockdown.
“All the wigs and dress-up outfits from every dress-up I have ever hosted (many) came out to help me become a number of simulated patients for three of our courses. Favourites were Zoya Lockdownikov (an extremely unsubtle Russian spy) and the Duchess of Covidshire in her sequinned hospital gown, who is always on the phone with various prime ministers and presidents.”
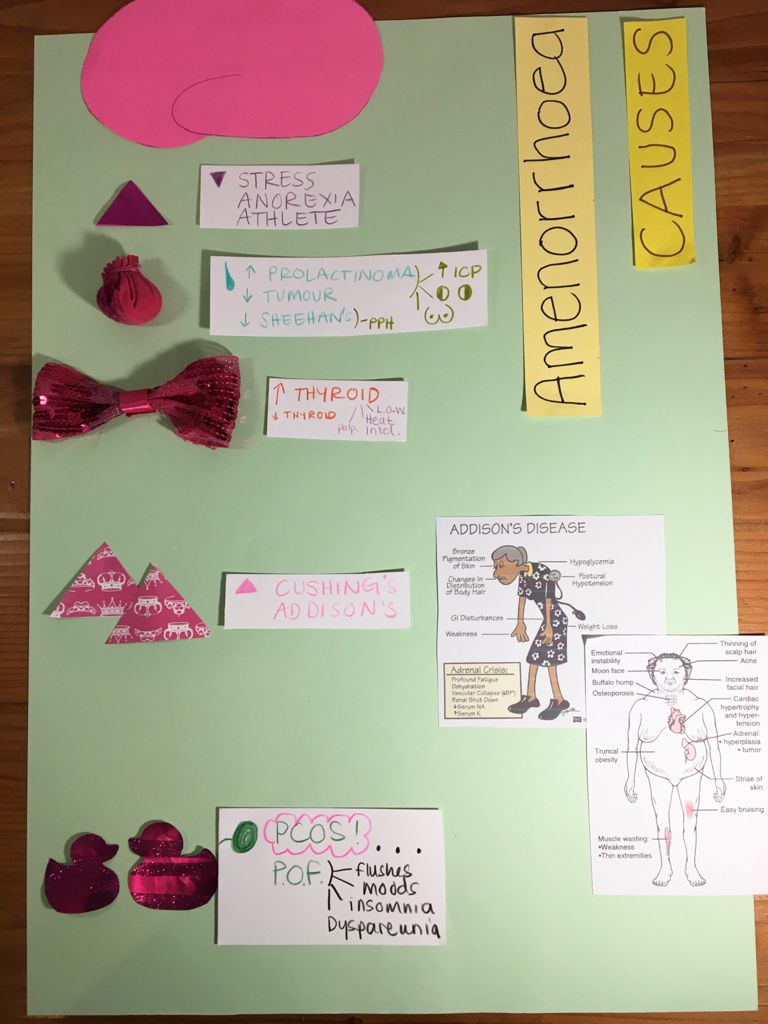
And so it began. There was very little to be purchased during hard lockdown, so whatever props were used had to come from the house. Every stuffed toy of my toddler’s had a role: every scrap of cardboard, all the tubs of glitter, crayons, antique telephones, and more. I remember hand-stitching a pituitary gland and a thyroid; making an endometrium with hair gel and red glitter; biopsying a potato; making tiny blood pressure cuffs for the stuffed toys; making a chicken hand puppet go into labour… and on and on… I also created quizzes for every single topic, which the students loved, but was incredibly time consuming for me.
.jpeg) The first course I had to design was for the fifth year gynaecology students. I learned a lot from this experience, so by the time the third year Women’s Health block came around, I was able to make a better product. Somewhere in the mix, the final year medical students returned to the platform, and because their exposure was so minimal, we decided to have Zoom tutorials with patient scenarios. This was later applied to the fifth year gynaecology students when they too returned.
The first course I had to design was for the fifth year gynaecology students. I learned a lot from this experience, so by the time the third year Women’s Health block came around, I was able to make a better product. Somewhere in the mix, the final year medical students returned to the platform, and because their exposure was so minimal, we decided to have Zoom tutorials with patient scenarios. This was later applied to the fifth year gynaecology students when they too returned.
Medicine wasn’t my only career choice - another strong contender was drama, and this served me greatly while working on the patient scenarios. All the wigs and dress-up outfits from every dress-up I have ever hosted (many) came out to help me become a number of simulated patients for three of our courses. Favourites were Zoya Lockdownikov (an extremely unsubtle Russian spy) and the Duchess of Covidshire in her sequinned hospital gown, who is always on the phone with various prime ministers and presidents.
I have never had so much fun at work in my life.
But, this was also in between volunteering in the COVID wards and some other clinical work, as well as trying to be present for a two-year-old. So, it’s also been a long time since I have felt this burnt out.
How did the students respond?
As someone with formal training in how to teach, I often get good feedback from students. But in my 8 years as an academic, I have never had such overwhelmingly positive rave reviews, especially from the third years. This group had to give anonymous feedback as part of their duly performed (DP) requirements. These students were robbed of their clinical exposure completely - they will not set foot into a Gynaecology ward in 2020, yet they raved about the online course. They were enthused; they were inspired; and they had learned. I received so many emails of thanks on top of the compulsory feedback. One afternoon, when Kirstenbosch had re-opened, two young women saw me there and shouted “Dr Gordon! We’re your third years!” and they came over to say hello and how much they had enjoyed Women’s Health. My heart soared.

What will come of this?
Firstly, I have been approached by the Faculty to make all of the content freely available as open access resources, and the Department of Health Sciences Education is busy designing a website, for which I have funding. Secondly, I presented two videos at the UCT Teaching and Learning Conference - one with my colleague Dr Emily Richardson, who also created many fabulous videos; and one with my husband, Dr Adalbert Ernst, who starred in several fabulous videos. Thirdly, I will never teach in the same way again – with a lecture theatre filled with more than 50 students while the lecturer goes through a ton of slides. I have a whole new vision of what face-to-face teaching time can be used for, and it’s going to be much more clinically-based, using the scenario videos. Finally, my IT skills have become exponentially better, and I doubt I will ever present at a conference in the same way as before either - videos all the way!
Acknowledgements
My colleagues and students know who they are, and they have been acknowledged where they have contributed. The person I really want to thank is Portia Maninjwa, our nanny, who did not hesitate to move in during lockdown so that I could create what I did. Enkosi kakhulu chomza!
Link to YouTube video: https://www.youtube.com/watch?v=Sd07_ifZOvU
 This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Please view the republishing articles page for more information.








